.png)
Is coronary artery calcification good or bad?
- Dr Edward Leatham
- May 28, 2024
- 6 min read

Updated: May 31
The evolution from calcium scoring to comprehensive plaque assessment demands a fundamental shift in how we stratify cardiovascular risk.
Read with full references & citations:
For busy people, or to tune in when on the move, a Google NotebookLM audio podcast is available as a story beneath.
Coronary artery calcification screening has transformed from an expensive curiosity to mainstream risk assessment, but our fixation on the Agatston score obscures more sophisticated approaches to plaque characterisation. The emergence of contrast-enhanced CT and fat attenuation index analysis offers unprecedented insight into plaque vulnerability. We must move beyond simple calcium detection to embrace comprehensive coronary risk assessment.
Background
The relationship between coronary artery calcification and cardiovascular risk represents one of the most significant diagnostic advances in preventive cardiology over the past three decades, yet it remains poorly understood by many clinicians who treat it as either reassuring evidence of plaque stabilisation or alarming confirmation of disease burden. This fundamental misunderstanding stems from viewing CAC through an oversimplified binary lens rather than recognising it as part of the complex continuum of atherosclerotic plaque evolution.
When I first encountered CAC scoring in the late 1990s, electron beam CT scanners cost several million pounds and occupied the space of a small aircraft hangar. The technology was revolutionary but prohibitively expensive, limiting its availability to a handful of research centres. Despite these constraints, landmark cohort studies demonstrated CAC's remarkable predictive power for future coronary events, with zero scores conferring excellent negative predictive value and higher scores showing strong correlation with subsequent myocardial infarction and cardiac death.
The mechanistic basis for this predictive power lies in understanding that calcium deposition represents the arterial wall's response to chronic inflammation and lipid accumulation. Calcium phosphate crystals form as part of the healing process following endothelial injury, effectively creating a protective shell around vulnerable plaque components. This process typically begins in the fourth decade of life, progressing predictably with age and cardiovascular risk factor burden.
However, the critical insight that only approximately ten percent of total plaque burden calcifies creates a diagnostic paradox. A patient with an Agatston score of 100 may harbour ten times that amount of non-calcified plaque, invisible to standard CAC protocols. This realisation has profound implications for risk stratification, particularly in younger patients or those with diabetes, where extensive non-calcified disease may exist despite minimal calcium deposition. The challenge for contemporary practice lies in moving beyond the false security of zero calcium scores while appropriately contextualising positive findings within the broader framework of plaque biology and patient-specific risk factors.
The Evidence
The evidence base supporting CAC screening emerged from several large prospective cohort studies, most notably the Multi-Ethnic Study of Atherosclerosis, which followed over 6,800 participants for more than a decade. MESA demonstrated that CAC scores provided incremental risk prediction beyond traditional Framingham variables, with hazard ratios for coronary events increasing from 2.1 for scores 1-100 to 9.7 for scores exceeding 400. The negative predictive value of zero calcium proved particularly compelling, with annual event rates below 0.1 percent in most populations.
The JUPITER trial indirectly validated CAC's clinical utility by demonstrating that rosuvastatin's dramatic benefits in reducing cardiovascular events were most pronounced in participants with detectable baseline calcium, supporting the concept that CAC identifies individuals most likely to benefit from intensive primary prevention. Subsequent post-hoc analyses showed number needed to treat values as low as 17 for patients with CAC scores exceeding 100, compared to over 100 for those with zero calcium.
However, the limitations of non-contrast CAC scanning became apparent through studies demonstrating significant coronary disease in patients with minimal calcification. The CONFIRM registry, encompassing over 27,000 patients undergoing coronary CT angiography, revealed that 13 percent of patients with zero calcium had non-calcified plaque, with 3.5 percent showing obstructive disease. This finding proved particularly relevant for younger patients and women, populations known to develop extensive non-calcified disease before calcium deposition occurs.
The development of fat attenuation index represents the next evolutionary step in non-invasive plaque characterisation. This technique measures inflammatory changes in perivascular adipose tissue, providing insight into plaque activity independent of morphology or calcium content. The CRISP-CT study demonstrated that elevated FAI values predicted future coronary events even after adjusting for traditional risk factors and plaque burden, with hazard ratios approaching 1.6 for each standard deviation increase.
Meta-analyses of CAC progression studies consistently show that calcium advancement follows predictable patterns, typically increasing 15-25 percent annually in patients with baseline disease. However, the clinical significance of progression rates remains controversial, with some studies suggesting faster progression paradoxically associates with better outcomes, possibly reflecting successful plaque stabilisation through calcium deposition.
Clinical Implications
The clinical application of CAC screening requires abandoning the simplistic interpretation of calcium scores as either good or bad news. Zero calcium in a 45-year-old patient with diabetes and family history cannot provide the same reassurance as zero calcium in a 55-year-old with optimal risk factors. Clinical decision-making must incorporate age-specific percentiles, with scores below the 25th percentile for age and sex providing meaningful negative risk stratification regardless of absolute values.
For patients with detectable calcium, the focus should shift from the specific Agatston score to the broader implications for preventive therapy. The evidence overwhelmingly supports intensive statin therapy for patients with CAC scores exceeding 100, with goals of LDL cholesterol below 70 mg/dL and consideration of non-statin therapies when targets prove unachievable. The common practice of using moderate-intensity statins based on intermediate risk scores represents a fundamental misapplication of the evidence base.
The integration of contrast-enhanced coronary CT into clinical practice demands careful patient selection and expertise in image interpretation. Unlike simple calcium scoring, coronary CT angiography requires consideration of radiation exposure, contrast nephrotoxicity, and downstream cascade effects from incidental findings. However, for patients with concerning symptoms and intermediate pretest probability, the ability to simultaneously assess calcified and non-calcified plaque provides unparalleled diagnostic information.
The emerging role of artificial intelligence in plaque analysis promises to revolutionise risk assessment by quantifying plaque characteristics invisible to conventional interpretation. Machine learning algorithms can identify subtle features associated with plaque vulnerability, potentially identifying high-risk patients before calcium deposition occurs. This technology demands integration into clinical workflows while maintaining the fundamental principle that imaging findings must be interpreted within the context of individual patient risk profiles and treatment goals.
Bottom Line
The evolution of coronary calcium assessment from research curiosity to clinical tool reflects our growing understanding of atherosclerotic plaque biology and the limitations of traditional risk factor assessment. The technology has matured from expensive electron beam scanners to widely available multi-slice CT systems, making risk assessment accessible to mainstream cardiology practice. However, the clinical application requires sophisticated understanding of plaque pathophysiology rather than simple score interpretation.
The evidence unequivocally supports CAC screening for risk stratification in intermediate-risk patients, with zero scores providing excellent negative predictive value and elevated scores identifying candidates for intensive preventive therapy. The limitations of calcium-only assessment have driven development of comprehensive plaque analysis incorporating non-calcified disease and inflammatory markers, promising more precise risk stratification.
Future developments will likely focus on artificial intelligence applications for plaque characterisation and integration of novel biomarkers for comprehensive risk assessment. The goal remains identifying patients most likely to benefit from preventive interventions while avoiding unnecessary testing in low-risk populations.
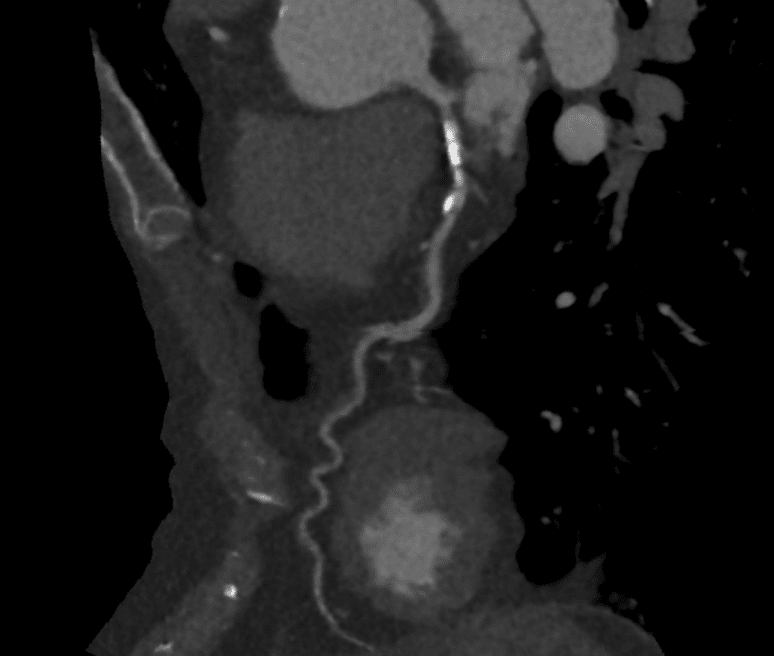
Case 1
The course of the LAD is shown by the contrast in grey, with focal coronary calcification in white. Workstation analysis showed no significant narrowing of the LAD.

Case 2
The course of the LAD is shown by the contrast in grey. Workstation analysis showed critical narrowing of the LAD.

Case 2 invasive coronary angiogram
An image of the invasive angiogram of case 2, taken a week later, confirming the CT findings. There is a severe narrowing (stenosis) affecting the left anterior coronary artery (LAD).
These images illustrate that although a raised CAC for age is associated with higher future coronary event rates, the absence of CAC does not exclude important coronary heart disease.
Key Takeaways
1. Zero calcium scores provide excellent negative predictive value but cannot exclude significant coronary disease in younger patients or those with diabetes who may harbour extensive non-calcified plaque.
2. CAC scores exceeding 100 identify patients who benefit from intensive statin therapy with LDL goals below 70 mg/dL, regardless of traditional risk calculator outputs.
3. Contrast-enhanced coronary CT offers superior plaque characterisation compared to calcium scoring alone but requires careful patient selection and expertise in interpretation.
4. Fat attenuation index analysis represents the next frontier in non-invasive plaque assessment, identifying inflammatory activity independent of plaque morphology or calcium content.
Summary
Coronary calcium screening has evolved from expensive research tool to mainstream risk assessment, but fixation on Agatston scores obscures sophisticated plaque analysis. Zero calcium cannot exclude disease in younger patients, while elevated scores demand intensive prevention regardless of traditional risk calculations.
Related Reading
1. Understanding Coronary Heart Disease: From Early Inflammation to Modern CT Imaging
2. What is FAI and how to interpret it?
3. Why FFR CT Heartflow?
4. Is coronary artery calcification good or bad?
5. Why I now might want to calcify my coronary arteries!


