.png)
BOOK 5 OF THE VAT TRAP SERIES
Do As You Would Be
Done By
A cardiologist's journey from intervention to prevention — and the most honest book in the series, because it's about my own scan.
From the Naked Heart series — making something complicated simple, but no simpler than the truth allows.
~180 pages 4-hour read. Coming 2026
THE CATH LAB, 2000
The room fell silent except for the flatline alarm.
"Thank you all for your efforts," I said. "I am so sorry."
We had been resuscitating for over an hour. Three hours earlier, the man on the table had been on the phone to me asking for advice about chest tightness after a run through the rain. Proud of our new Rapid Access Chest Pain Clinic, I had invited him straight in. A stress ECG showed the tell-tale pattern. An urgent angiogram was the next step.
What we did not know was that he had only one major coronary artery supplying his heart, and that the act of performing the angiogram itself would disturb the plaque inside it. The artery occluded. Without an emergency angioplasty service on site, there was nothing we could do.
He was a friend.
That night, at home with a stiff gin and tonic, I made a promise to myself — that there must be a better way to detect dangerous coronary anatomy before it killed people. A non-invasive way. An accurate way.
What followed was, in the secular sense, my road-to-Damascus moment: the day my career changed direction without me noticing for several more years.
THE PROMISE KEPT
Eighteen years later, the same answer arrived in a different form.
Six years after that night, in 2006, I shook hands with a consultant thoracic radiologist and we launched one of the NHS's first joint cardiac CT angiography services. Then, with a bank loan, I leased a unit next door to Lifescan in the Surrey Research Park — already pioneering CAC scoring on a 16-slice CT — and founded what would become Surrey Cardiovascular Clinic, dedicated to early diagnosis and prevention.
Eighteen years after the cath-lab death, I knelt beside a taxi driver who had collapsed in ventricular fibrillation during a routine occupational stress ECG. He had no symptoms. He had only walked in because his council required it to renew his licence. As the defibrillator charged, I remembered the promise.
We now had a cardiologist-led CT service we called the virtual cath lab — capable of identifying dangerous coronary narrowing with millimetre precision, quantifying plaque burden, sending scans to Stanford for flow analysis, to Oxford for inflammation imaging, and detecting disease decades before symptoms appeared.
The taxi driver walked out of the clinic that day alive, escorted by paramedics, to applause from the waiting room. Four weeks later he came back, post triple-bypass, to shake my hand.
The promise had been delivered.
But I had no idea what was coming next.
And then I looked at my own
scan.
THE CARDIOLOGIST BECOMES THE PATIENT
Thirty years treating heart disease one artery at a time
I followed the orthodoxy: statin, 10,000 steps a day, the lot. And the middle-age spread did not budge. When my own CT showed a high fat attenuation index — matching, almost exactly, a patient my age who had just had a heart attack — my first reaction was denial.
The arthritis that finally stopped me walking pushed me into yoga and acupuncture, which only made it worse. Only then, almost reluctantly, did I try a micro-dose of a GLP-1.
The pain went. The waist went. The visceral fat went — documented on serial VAT-CT measurements, twelve weeks apart.
VISCERAL FAT (VATI)
BODY WEIGHT
WAIST CIRCUMFERENCE
41 34 cm / m
2
2
102 92 Kg
110 96 cm
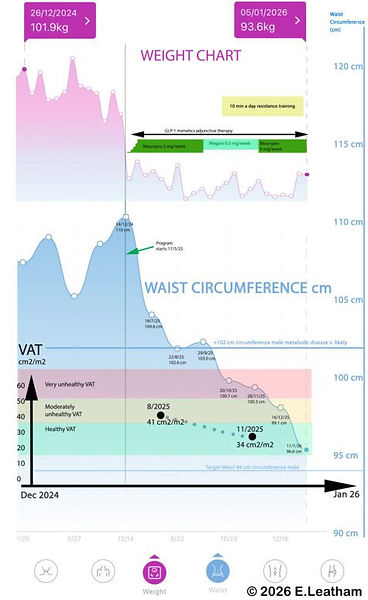
It was not the weight that mattered. It was the visceral fat — the marker no one had measured before, and the one that explained everything else. The cardiologist had become the first patient.
DISCOVERIES ALONG THE WAY
What started as a personal experiment turned into a research programme I had not planned.
Patients were walking into clinic with Zoe and continuous glucose monitor data, asking what it meant. I tried a CGM myself — and what came next reshaped how I practise.
I
II
III
IV
V
VI
The baked potato that hit 13 mmol/L
A healthy lunch on a busy clinic day after a poor night's sleep sent my own glucose to thirteen. Half the patients we then tested spiked the same way. Most of them had no idea they were even at risk.
Four siblings, three prediabetic HbA1cs
A quiet check of my own HbA1c, and then my three sisters', revealed all four of us in the prediabetic range no one had ever told us about. Carbohydrate sensitivity, it turned out, ran in the family — another quiet example of epigenetics shaping risk decades before disease appears.
HbA1c returned to normal in six months
We started flattening the glucose curve. Six months in, every HbA1c in the family had dropped - 2 of 3 siblings back into the normal range — without medication, without dramatic intervention, just by recognising what each of us was actually sensitive to.
The Virta question I still can't answer
I came across Virta Health in the US — peer-reviewed evidence of 60% Type 2 diabetes reversal, sustained HbA1c reductions, insulin de-prescription in some patient groups. And I asked the obvious question that the book sets out to answer: why isn't this mainstream?
Strength is not the same as bulk
After a GLP-1 microdose I added ten minutes of resistance training, five days a week. Bioimpedance scales said I was losing muscle mass, and I nearly stopped — until I realised that dynapenia (functional weakness) predicts poor outcomes after sixty more strongly than sarcopenia (low muscle mass), and that the bulk "lost" on a GLP-1 is largely glycogen and intramuscular fat. My strength was rising — a 3 kg outstretched-arm hold to 10 kg over eight months — even as the scales said the opposite.
Ten minutes a day beats the gym membership abandoned in March
The longevity-author orthodoxy makes heavy weightlifting non-negotiable. Sound advice for the small minority who will sustain it for twenty years; less useful for the majority who won't. My own programme — 10,000 steps, no running (to spare the joints), and ten minutes of all-body strength training daily — produced a VO₂max in the 95th centile for age at sixty-four. The interventions that move the needle are the ones you can still be doing in 2031.
THE ARC
From Cardiology 1.0 to Cardiology 3.0 — through one career
Book 5 traces the evolution of cardiology from the catheter lab to the CT scanner across thirty years of one consultant's practice — from intervention, to imaging, to honest measurement of the things that actually drive disease.
Cardiology 1.0
SYMPTOM ERA
Treated heart attacks once they arrived. Diagnosis followed crisis.
Cardiology 2.0
INTERVENTION ERA
Got better at stenting blocked arteries. Saved lives — but still arrived too late.
Cardiology 3.0
PREVENTION ERA
Sees risk early enough to do something about it — using imaging, AI, metabolic measurement, and an honest understanding of what actually drives disease.
WHO THIS BOOK IS FOR
The most personal book in the series
Book 5 is the backstory of how we got here. Stepping back from the NHS in 2021 gave me what thirty years of high-volume practice never had: time to measure, to read, and to follow the trail wherever it led.
READ THIS BOOK IF
-
You've read Books 1–4 and want to understand how the framework was built
-
You are a patient of mine and want the longer story behind the protocols
-
You're a clinician interested in how one consultant moved from intervention to prevention — and what it cost
-
You've ever wondered why some of the most effective treatments in metabolic medicine remain outside mainstream guidelines
-
You appreciate a memoir that doesn't flinch from the writer's own data
THIS BOOK IS NOT FOR
-
Anyone in a hurry — Book 1 will give you the framework faster
-
Readers wanting a how-to manual — that's Books 2 and 3
-
Anyone uncomfortable with a doctor talking openly about his own metabolic problems
Not every reader will need this book. Some of my patients will. So might anyone who has ever wondered why the answers seem to lie just outside the system that is supposed to provide them.
STAY INFORMED
Be told when Book 5 is published
Register your interest. You'll receive early extracts as they are written, plus the weekly journal posts that explore the same questions in real time.